
I remember when my dad told me that there was no such thing as Santa Claus. He sat me down and told me that it had been him all these years who had been buying me gifts and placing them under the tree. It was quite a shock to have this revealed to me; it shook my world. I did everything in my power to reason it through. In my head, dad was a liar. Dad wanted to take the credit for the big jolly guy who’d given me all the gifts I’d ask for in the letters I sent him through my dad.
I was 27 years old.
Soon enough, I came to accept the truth. All the evidence was there in the form of my dad’s receipts for the gifts he had gotten me. People had seen him buy me those gifts. Mom swore to having helped him wrap them. The evidence was compelling, substantial, tangible, credible… Santa Claus was no more.
I’m sad to say that this is not the case with the anti-vaccine crowd. You can tell them all you want that vaccines do not cause autism, and that vaccines actually protect from diseases that are deadly and/or disabling. But they will refuse to believe it because their entire ecosystem depends on the belief that vaccines cause autism. Anything short of that sucks away their life, their reason for living.
One such anti-vaccine zealot is everyone’s favorite “kid.” Even with a master of public health degree in epidemiology, he seems to remain convinced that vaccines cause autism. He’s stated on his blog that evidence he saw in school to the contrary is all a conspiracy from the pharmaceutical industry. It seems that, to him, the lies he has been exposed to over and over from a very young age have made up his mind. To him, Santa Claus (i.e. vaccines cause autism) still exists, and it will continue to exist because anything short of that eliminates his reason for living.
Seriously, he doesn’t seem to live for anything other than that. The primary example is a recent blog post of his where he takes a study that clearly shows that the Tdap (Tetanus, Diphtheria, and acellular Pertussis) vaccine doesn’t cause autism, and then he states that the study confirms that the influenza vaccine does cause autism.
Yeah, I was confused too.
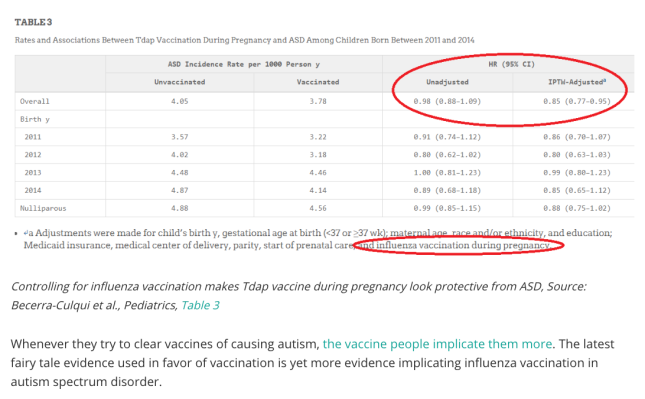
His whole argument hinges on one table in the Prenatal Tetanus, Diphtheria, Acellular Pertussis Vaccination and Autism Spectrum Disorder by Becerra-Culqui et al.
This is table 3:

Table 3 states that women who were vaccinated with Tdap during pregnancy had a similar incidence rate per 100,000 person-years of having an autistic child. Vaccinated women had an incidence rate of 3.78 autistic children per 100,000 person-years while un-vaccinated women had an incidence rate of 4.05. The ratio between the two was 0.98, meaning that vaccinated women had a lower incidence rate than vaccinated. Anything over 1.0 would indicate that vaccination leads to more autistic children being born.
Because this is one study with a limited number of people, and not a study looking at the entire universe of children born, scientists also report the 95% confidence interval (0.98 – 1.09). The 95% confidence interval is a way of us saying, “We are 95% confident that the true hazard ratio in the entire population (the whole of the population) is between 0.88 and 1.09.” Because it includes 1.0, we cannot say that this observation is not by random chance.
But look at how the kid displays the table on his blog:
Only point out the things that seem to support your argument.
He points out that the adjusted hazard ratio of 0.85 (with a 95% confidence interval of 0.77 to 0.95) is adjusted for, among other things, influenza vaccination during pregnancy. In epidemiology and biostatistics, “adjusted for” means taking it into consideration. Let me give you an example:
Suppose that there are a group of people from Texas and a group of people from Alabama, and that we look at their test scores in biology. The group from Texas had an average test score of 77% while the people from Alabama had an average test score of 89%. You would conclude that being from Alabama leads you to having a better test score, right?
But what if we told you that they don’t teach biology in all schools in Texas? What if we told you that they only teach it in private schools in Texas, and that only 30% of schools in Texas are private schools? And then we told you that they teach biology in both types of schools in Alabama, and that there is a 50-50 split in the proportion of private to public schools in Alabama? How does this change your conclusion?
To reach the proper conclusion, you have to compare apples to apples, and oranges to oranges. You would compare the private school scores in each state to each other, and likewise with the public school scores. This is an adjustment. This is taking into account the differences in the distributions of a characteristic between the two groups being studied.
As it turns out, in the study in question, women who get their Tdap were much more likely to get their influenza vaccine. It makes sense, right? Women who vaccinate in general are more likely to vaccinate in particular. So, in order to compare apples to apples, the researchers adjusted for influenza vaccination. That is, they compared flu-vaccinated women who got the Tdap and flu-vaccinated women who did not get the Tdap, AND non-flu-vaccinated women who got the Tdap and non-flu-vaccinated women who did not get the Tdap.
Taking flu vaccination into account, and the bias that would creep in because women who vaccinate against influenza seem to be more likely to vaccinated with the Tdap vaccine, vaccinating with Tdap is not associated with having a child diagnosed with autism.
So why does the kid think this proves that influenza vaccine causes autism?
It beats me. All they did was make the adjustment to make things equal between the two groups, something every epidemiologist worth their salt should do… Unless you want to misinform the public?
Hmmmm?
He then takes a table from a different, unrelated study and points out to just one result on it as evidence that influenza vaccine causes autism:

The red circle seems to be his way of saying, “Only this matters! Pay no attention to the whole of the evidence!”
This is another misrepresentation of the findings, and I kind of blame the authors of the study for making the table so busy. Look at the “Variable” column on the left. All that the data circled in red are saying is this:
“Of the 13,477 children whose mothers were vaccinated in the first trimester, 258 (1.91%) of them were diagnosed with autism. Their hazard was 26% higher for an autism diagnosis when compared to children whose moms were vaccinated in other trimesters. However, when adjusting for maternal allergy, asthma, autoimmune conditions, gestational diabetes, hypertension, age, education, race/ethnicity, child conception year, conception season, sex, and gestational age, the hazard of autism diagnosis went down to 20% over children whose moms were vaccinated in other trimesters.”
The fact that the hazard ratio went down after adjusting tells us that there is something else explaining the elevated hazard (risk). Look at what happened in the adjustment in the other trimester groups… Nothing changed. Look at what happened in the adjustment in the “Anytime During Pregnancy” group… Nothing changed. So what could that “something else” be? I’m not an obstetrician, but it’s reasonable to conclude that outcomes measured in the first trimester are different than outcomes measured in the other trimesters.
Finally, look at the reasoning that the kid used. In the first table, because numbers were adjusted for influenza vaccination, then it must mean that influenza vaccination causes autism. In the second, he doesn’t say that all the factors adjusted for cause autism… Because that would tear down his narrative.
I’m not surprised at all by his misunderstanding of all this. After all, to my knowledge, he doesn’t work as an epidemiologist anywhere. Like any good muscle, lack of practice of your epidemiology skills leads you to lose them. Being unpublished, not working as an epidemiologist, and a staunch defender of the so-called autism-vaccine risk leads the reasoning muscle to atrophy.



